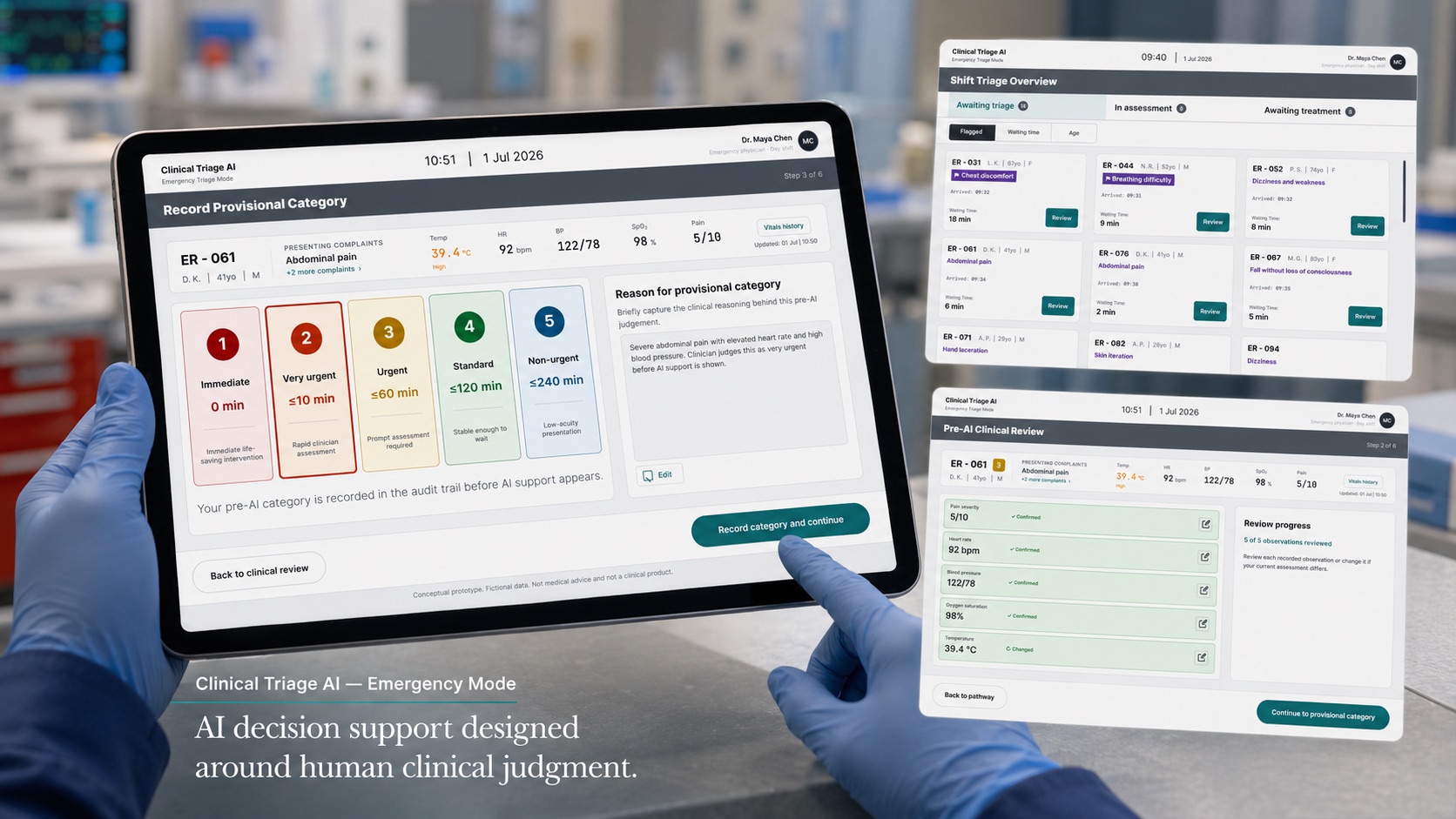
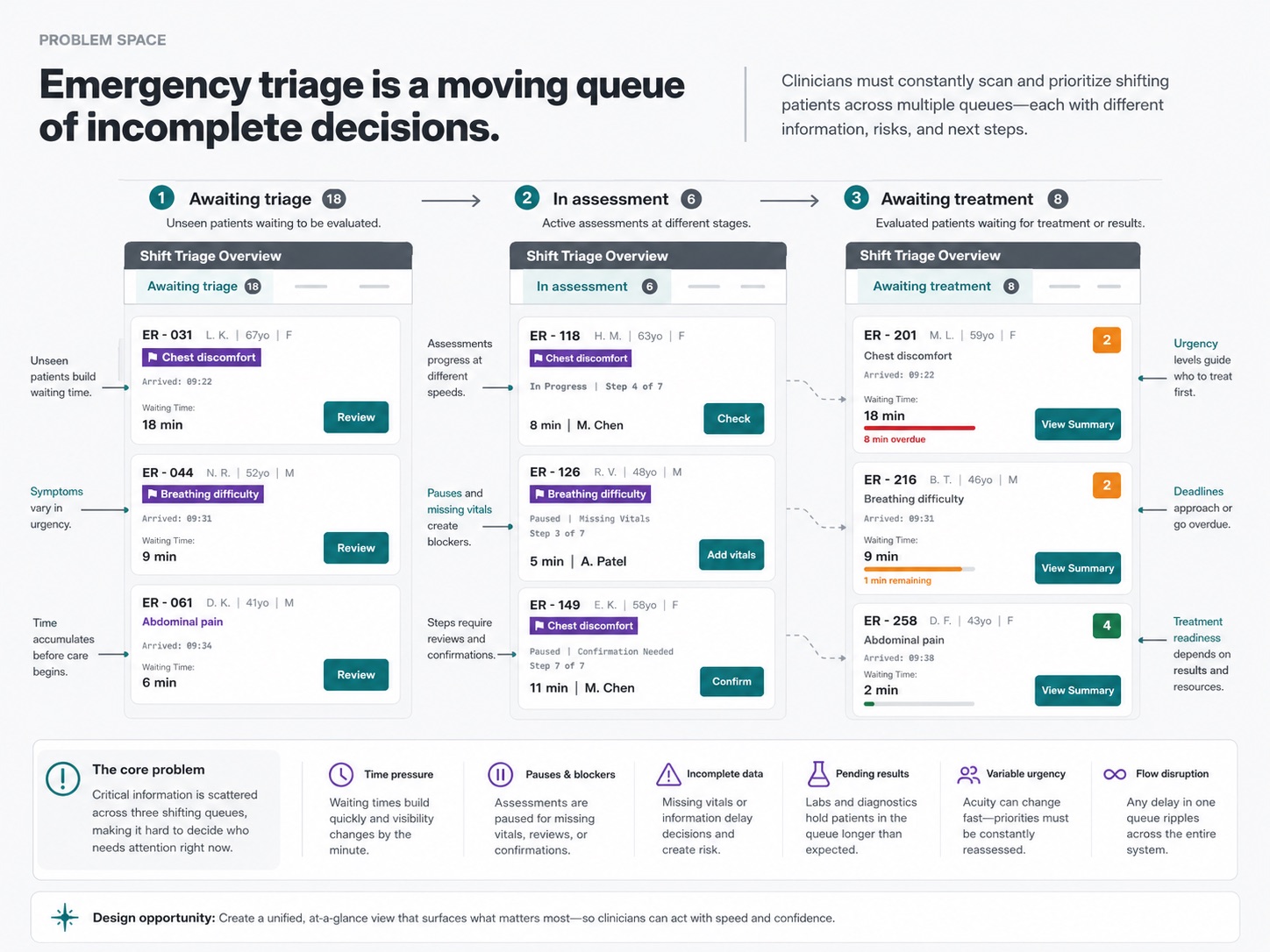
Reviewing before the machine does
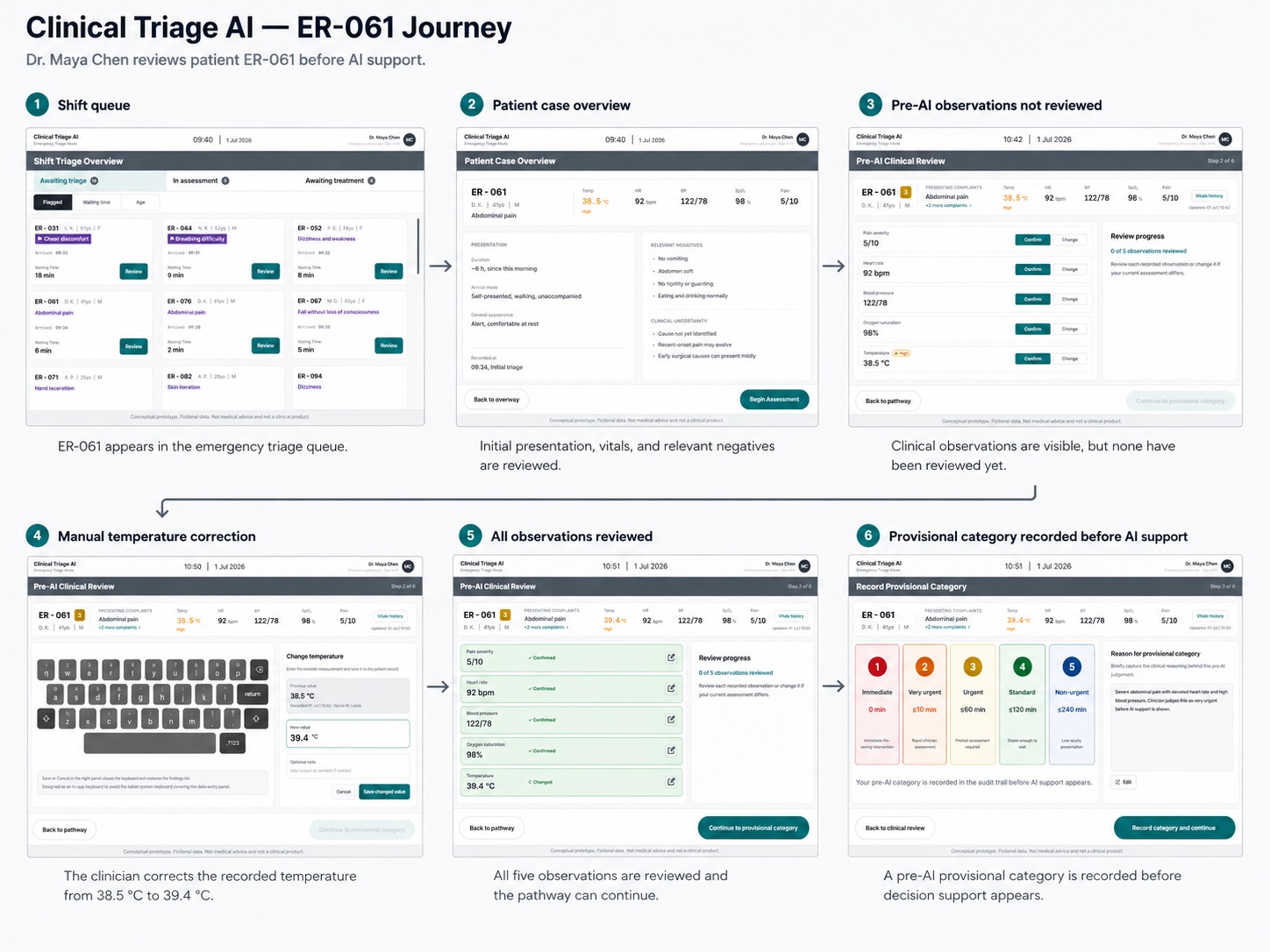
Before Dr. Maya Chen can see any AI input on patient ER-061 (41-year-old male, abdominal pain), she has to review five clinical observations one by one — confirming or correcting each. Nothing moves forward until this step is complete.
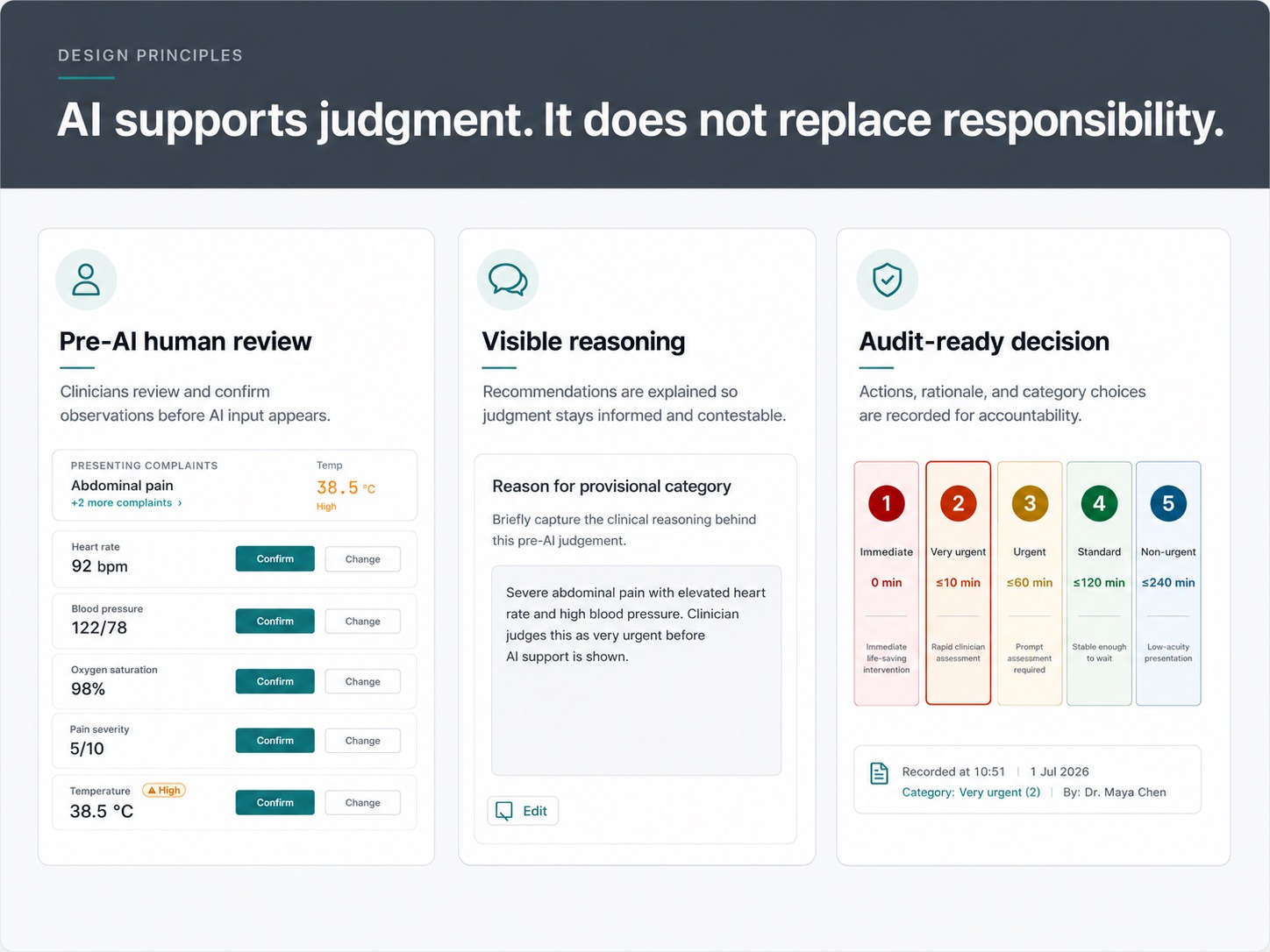
The Decision
The system requires explicit confirm/change on each observation rather than defaulting to “auto-accept unless flagged” — a faster pattern that would have skipped forcing genuine clinical attention onto each value.
What I Learned
A small interaction detail — an in-app keyboard that doesn’t let the tablet’s system keyboard cover the data panel — turned out to matter as much as the AI-sequencing decision itself. Clinical software lives or dies on bedside mechanics like this.
Looking Forward
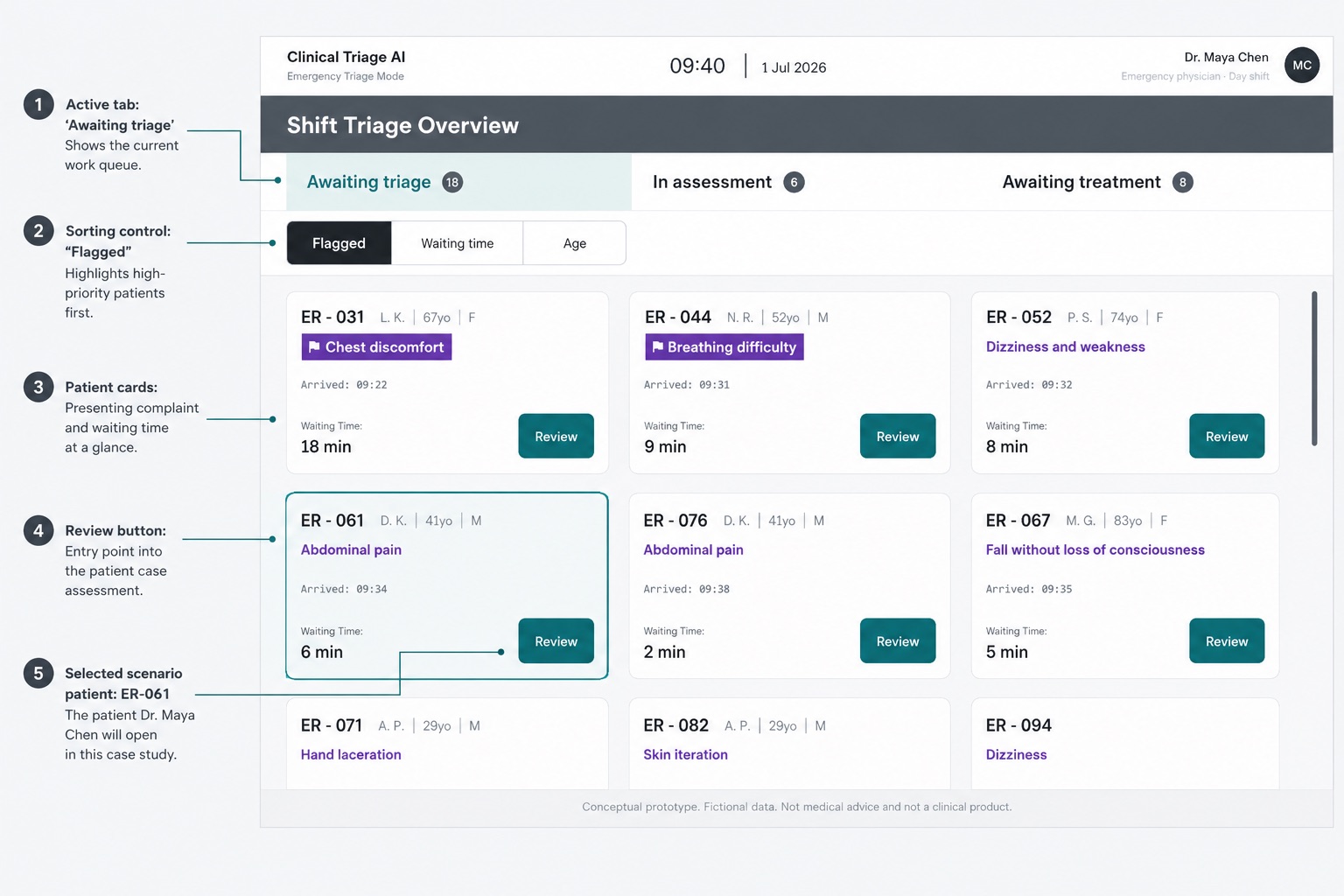
Whether this five-observation review actually feels necessary to a working clinician, or like friction, is the first thing worth testing with real users.